The lifetime risk of developing dementia after age 55 sits at roughly 42%, a number that sounds like a verdict rather than a statistic. But the history of research into age-related cognitive decline tells a very different story than the one most people carry around in their heads, and understanding why common belief is wrong about age-related cognitive decline requires looking at where that belief came from in the first place.
For most of the twentieth century, the working assumption in medicine was simple. Neurons peaked in young adulthood and declined steadily afterward, with nothing much to be done about it.
That assumption came from limited data, cross-sectional studies, and a scientific culture that hadn’t yet mapped structural plasticity or neurogenesis in the adult brain. It became common belief because it was repeated, not because it was proven.
The problem is that this old story still shapes how most people think today, in 2026, even though the evidence underneath it collapsed decades ago.
The modern picture is different, and it’s not vague optimism. It’s measurable.
Neuroplasticity Solutions was founded on a simple but radical premise: the brain you have today is not the brain you are stuck with. That premise now sits on a substantial body of published research, not a slogan.
Cognitive decline correlates with age, but correlation is not the same as biological inevitability. Lifestyle factors, training intensity, cardiovascular health, and social engagement all move the needle in ways that pure aging models never accounted for.
Researchers have gone as far as challenging the popular claim that lifestyle changes can prevent 45% of dementia cases, calling this figure a “theoretical maximum” for entire populations rather than a promise for any one individual. That nuance matters. It means the modifiable-risk story is real, but it isn’t a marketing slogan either.

New research shows a striking share of dementia risk traces back to factors people can actually change, not just aging itself.
Here is where common belief and current evidence really diverge. Nearly all U.S. adults over 40 say brain health matters as much as physical health.
But saying it matters and knowing what to do about it are two different things entirely.
That 90-point gap is the same gap Neuroplasticity Solutions was built to close. We call it the research-to-practice gap, and it’s the reason why common belief is wrong about age-related cognitive decline in practically every direction, not just one.
People overestimate how inevitable decline is, and simultaneously underestimate how specific the intervention needs to be to change it.
Most of what gets marketed as “brain health” skips the actual biological target entirely. We don’t.
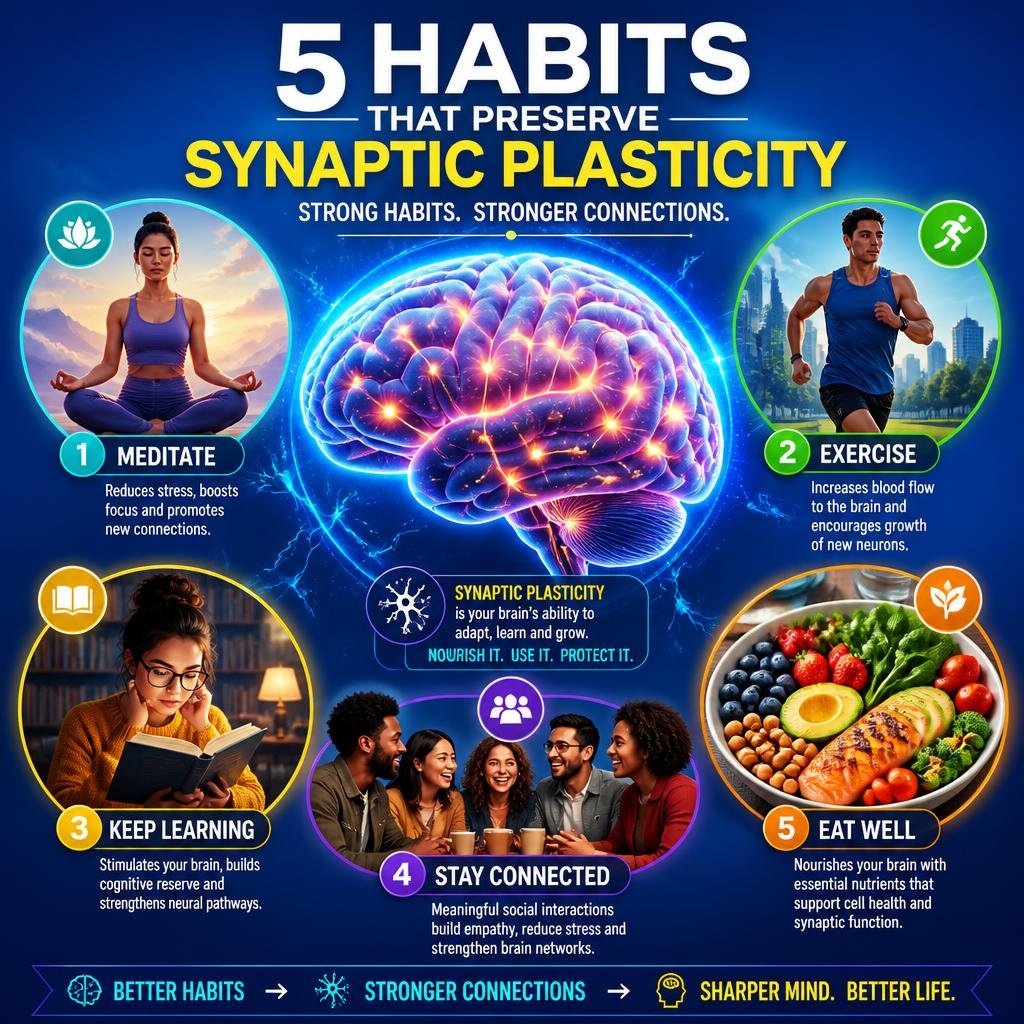
We treat Brain-Derived Neurotrophic Factor as your brain’s repair protein, supported by training, movement, and lifestyle, not by wishful thinking. BDNF is involved in neurogenesis, synaptic strength, and the structural plasticity that lets the adult brain keep adapting well past the age most people assume is a ceiling.



Our guide to activating your brain’s BDNF walks through the 40Hz gamma audio approach alongside training and movement inputs, because BDNF doesn’t respond to a single lever pulled once. It responds to consistent, correctly dosed stimulation, and that’s a very different proposition than “aging is just aging.”
Not all brain-focused tools are built equally, and the difference between a casual memory app and a real cognitive training program matters enormously for attention and long-term cognitive maintenance.
The U.S. POINTER Study, published in 2026, found that seniors in structured lifestyle interventions performed at a level comparable to adults one to two years younger than those relying on self-guided methods. That single data point should change how anyone thinks about cognitive training versus memory apps for older adults.
Static difficulty, predictable puzzles, and passive scrolling through trivia don’t meet the threshold that produces measurable change. The brain only adapts meaningfully at the edge of current ability, which means:
Evidence over enthusiasm. You need measurable progress, not vibes, and a puzzle app that never adjusts difficulty cannot deliver that no matter how many hours you put into it.
If cognitive decline were truly a fixed, one-way slope, stroke rehabilitation wouldn’t work at all. It works, and the mechanism explains a lot about why age-related decline isn’t the closed case common belief assumes.

Constraint-Induced Movement Therapy (CIMT) is one of the most rigorously studied approaches to post-stroke motor recovery. It forces the brain to recruit surviving tissue by restraining the unaffected limb for several hours daily, combating learned non-use and pushing reorganization of motor networks that were assumed dormant.
Mental practice and motor imagery work on a related principle. Deliberate visualisation activates similar cortical networks as the actual movement itself, which is exactly the kind of structural plasticity that “brains just decline with age” fails to explain.
CIMT is not suitable for every patient and needs to be designed by a clinician within a multi-modal rehabilitation framework, not attempted alone. But the fact that it works at all, in adult and aging brains, is direct evidence against the fixed-decline model.
You cannot argue with common belief using vibes. You argue with it using numbers, and cognitive assessment has gotten considerably more precise about catching early change.
The Mini-Mental State Examination (MMSE) has been the standard screening tool for decades, but it can miss early cognitive changes in higher-functioning individuals. The Montreal Cognitive Assessment (MoCA) is typically more demanding and detects Mild Cognitive Impairment with greater sensitivity, which is why clinicians increasingly reference our MoCA to MMSE score conversion chart when tailoring training and rehabilitation plans.
Separately, there’s the distinction between brain age and chronological age, a metric that quantifies exactly how much of “decline” is actually attributable to years lived versus modifiable biological factors. Our breakdown of brain age versus chronological age covers how this gap is measured and, more importantly, how it moves.
The supplement market is where the loosest claims live, and it’s also where the biggest gap sits between what’s marketed and what’s actually supported by evidence.
That silence between patients and providers is exactly the space where unverified nootropic claims fill in the blanks. Our guide to cognitive performance supplements exists to close that gap with the same evidence-first filter we apply to every protocol.



The point isn’t that supplements are a shortcut around training. They’re not. Used alongside structured protocols and movement, certain compounds can support the same BDNF pathways we already discussed, but they never replace dosing principles that come from actual training intensity.
Modern neuro-rehabilitation is no longer guesswork. It’s a measurable process built on rigorous evidence, clear dosing principles, and real follow-through.
Neuroplasticity Solutions grew out of a frustration shared by clinicians, researchers, and clients alike: the public market was full of noise, and the peer-reviewed literature rarely reached the people who needed it. Every protocol we deliver is grounded in published research and adapted to the individual in front of us, not a generic profile, not a marketing persona, but a specific person with specific goals, a specific history, and a specific brain.
You will never hear us promise to reverse ageing or unlock 100% of your brain. Those phrases belong in marketing copy, not in a clinical setting, and they’re part of why common belief is wrong about age-related cognitive decline in the first place. The belief was built on either fatalism or hype. The evidence sits in the middle, and the middle is where actual progress happens.
The history here is short but clear. Decades of assuming the brain only declines with age gave way to a body of evidence showing structural plasticity, neurogenesis, and BDNF-driven repair continue well into later life, provided the input is specific enough and dosed correctly.
Whether you are a high-performing professional looking to sharpen your edge, a senior aiming to preserve memory, or someone recovering from a neurological event, understanding why common belief is wrong about age-related cognitive decline is the first step toward a proactive roadmap for cognitive longevity, not a passive one.
No. While some changes in processing speed are statistically common with age, research on structural plasticity and neurogenesis shows the adult brain retains the capacity to adapt, repair, and even improve specific functions with the right training and dosing.
Public knowledge has lagged far behind the science. Nearly all U.S. adults over 40 say brain health matters, yet only a small fraction say they actually know how to protect it, which keeps outdated fatalism alive.
Casual memory apps with static difficulty and passive trivia rarely produce measurable change. Structured cognitive training programs that adjust difficulty and dose intensity correctly have shown stronger, evidence-backed results in 2026 research like the U.S. POINTER Study.
Brain-Derived Neurotrophic Factor is often described as the brain’s repair protein, supporting neurogenesis and synaptic strength. It responds to consistent training, movement, and lifestyle inputs, which is a major reason age-related decline is more modifiable than commonly believed.
No. Age-related cognitive changes and dementia are different, though subjective cognitive decline can sometimes be an early indicator. Assessment tools like MoCA and MMSE help clinicians distinguish normal aging patterns from signs that warrant closer monitoring.
Yes. The fact that constraint-induced movement therapy and motor imagery training can remap function in the adult brain after a stroke is strong evidence against the idea that the brain is fixed and only declines with age.
Supplements can support the same biological pathways involved in BDNF production, but they work best alongside structured training, not as a replacement for it. Evidence-based use, not marketing claims, should guide any decision here.