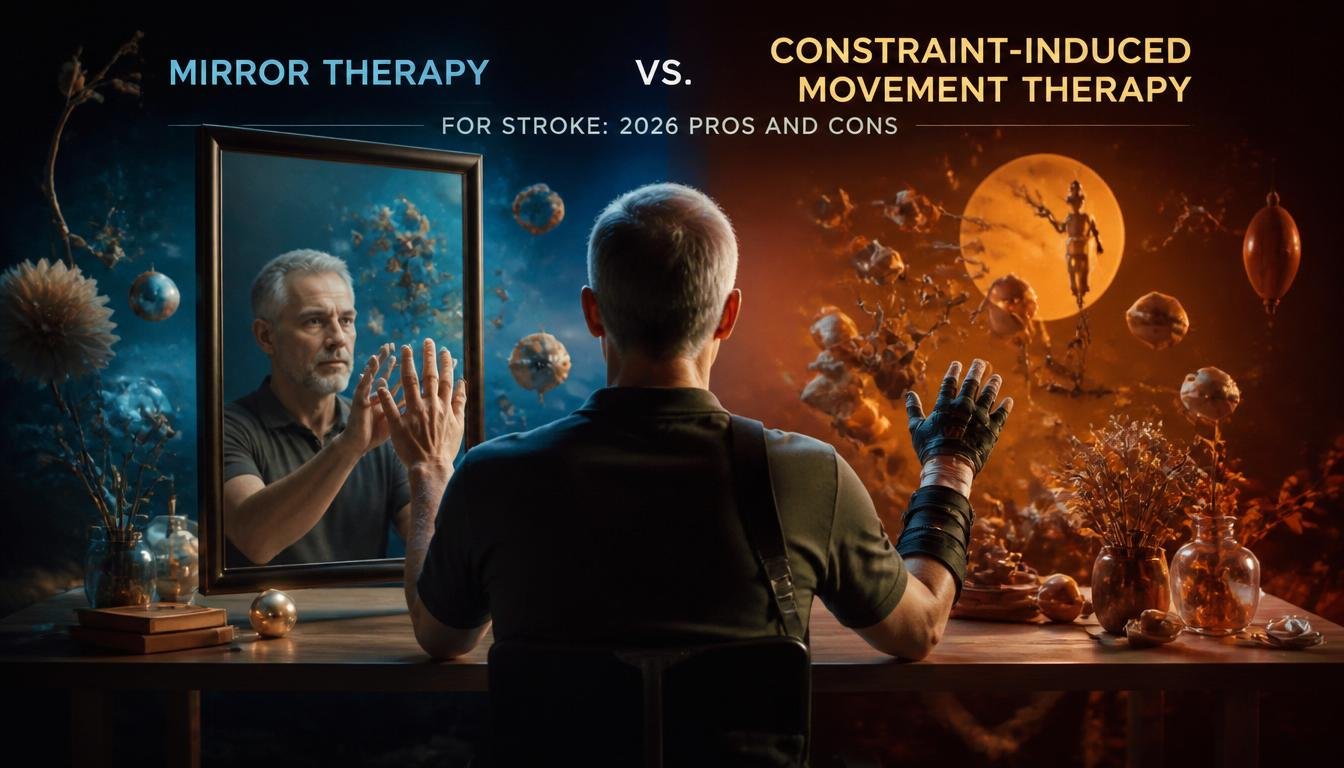
Did you know that only 5 to 20% of stroke survivors achieve functional capacity in their upper limbs? This stark reality makes the clinical debate around Mirror Therapy vs Constraint-Induced Movement Therapy for Stroke highly relevant in 2026. The brain is a biological system, not a motivational one. Good intentions do not rebuild neural circuits.
To understand how these modalities fit into a broader clinical framework, you can explore our neuro rehabilitation programmes.
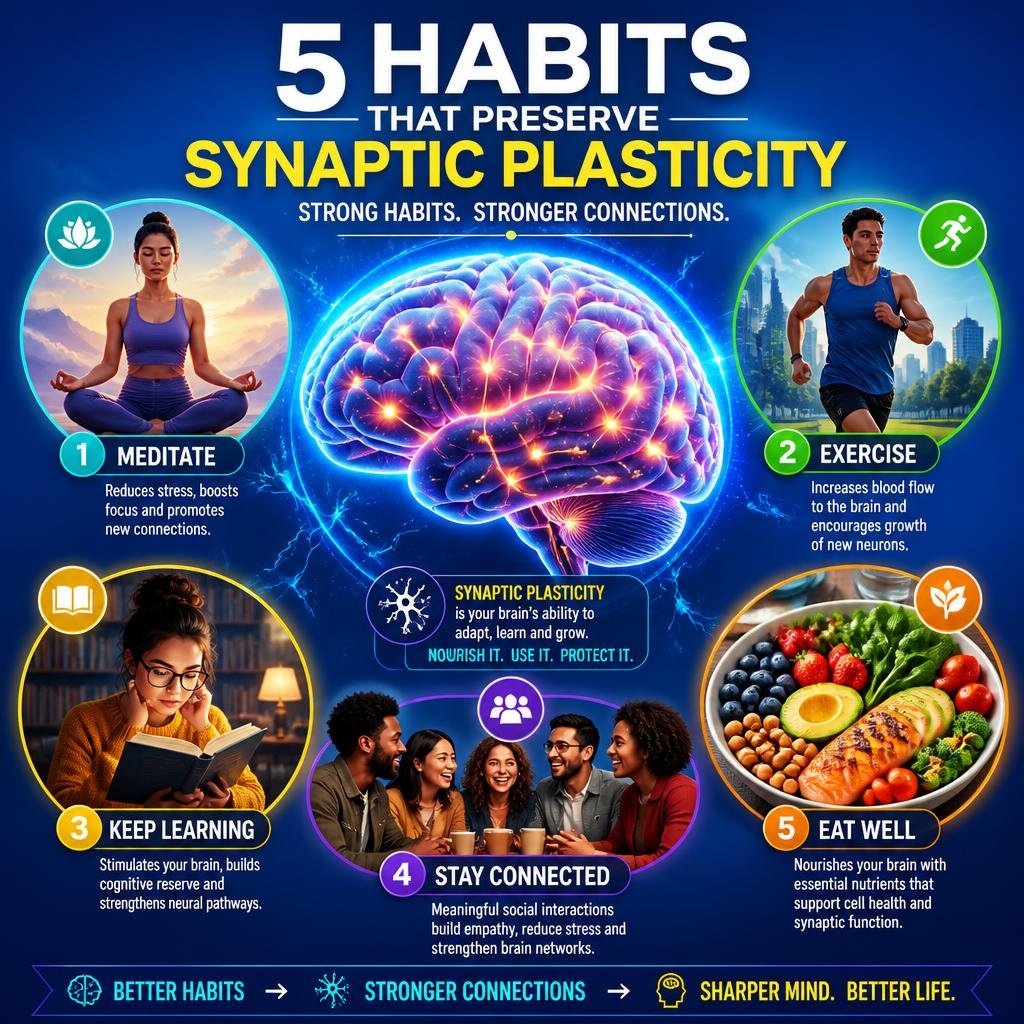
The brain you have today is not the brain you are stuck with. Stroke recovery hinges on neuroplasticity, the brain’s ability to rewire itself after damage. When we look at Mirror Therapy vs Constraint-Induced Movement Therapy for Stroke, we are looking at two different ways to force that rewiring.
Mirror Therapy involves placing a mirror between the patient’s arms. The patient moves their unaffected arm, and the mirror creates the illusion that the affected arm is moving normally. This visual feedback stimulates the motor cortex.
Constraint-Induced Movement Therapy (CIMT) takes a different approach. We restrain the unaffected limb, usually with a mitt, forcing the patient to use their affected arm for daily tasks. The goal is to overcome “learned non-use,” a phenomenon where the brain simply stops trying to use the damaged limb.

Both therapies offer distinct advantages depending on the patient’s current threshold-of-ability. Brain conditioning is more like going to the gym than taking a magic pill. You need the right tools for the right stage of recovery.
Neuroscience is an exciting field, and that excitement sells. We cut through the hype to look at the limitations of each protocol. Meaningful neuroplastic change is not a subscription you scroll through on your phone.
Addressing only one input while ignoring the others is leaving gains on the table. Both Mirror Therapy vs Constraint-Induced Movement Therapy for Stroke depend on a crucial underlying mechanism: BDNF activation. Brain-Derived Neurotrophic Factor is the repair protein that allows your brain to form new synaptic connections.
Without adequate BDNF, your brain lacks the structural plasticity needed to lock in motor gains. This is why we recommend a priming window before physical therapy. Using 40Hz gamma audio stimulation triggers your brain’s natural BDNF production.
You can prime your nervous system with the Genius Switch audio series. This creates the optimal biological environment for motor relearning. Think of it as Miracle-Gro for your brain, preparing the soil before you plant the seeds of motor repetition.
Results require daily repetition, focused listening, and a quiet environment. The difference between a successful recovery and a stagnant one often comes down to dose and intensity. When evaluating Mirror Therapy vs Constraint-Induced Movement Therapy for Stroke, intensity is the dividing line.
Mirror therapy is easy to dose but hard to scale. CIMT is difficult to dose but highly scalable. The modified CIMT protocol scales back the 6-hour daily requirement to 30 minutes of intense therapy combined with a restraint worn for most of the waking day. This makes it accessible for outpatient or home-based neuroplasticity tools.

While highly effective for upper limb recovery, Constraint-Induced Movement Therapy demands a rigorous daily commitment.
The gap between a conventional outpatient clinic and a neuroplasticity-integrated program is measurable in motor function scores. When we track outcomes for Mirror Therapy vs Constraint-Induced Movement Therapy for Stroke, we look for structural plasticity, not just temporary functional improvements.
CIMT forces the brain to confront its deficits. It demands high cognitive load and physical exertion. This is the kind of stress that drives structural changes in the brain.
Mirror therapy can support these changes, but it rarely drives them independently. We use it as a supplementary tool. It helps prime the motor cortex for the heavier work that CIMT requires.
If we cannot show you that something is working, we have no business recommending you continue it. We use cognitive assessments and motor mapping to verify that the protocol is actually rewiring your brain. If the data does not move, we change the protocol.
Choosing between these modalities is not an either-or decision. It is a multi-modal approach. You start with what your nervous system can handle right now.
If you have severe flaccidity, start with Mirror Therapy and BDNF activation. Once you achieve active wrist extension, you graduate to modified CIMT. This is how you build cognitive performance and motor capacity.
We treat recovery as an industrial process. You do not build a house by randomly swinging a hammer. You follow a blueprint. Our clinical-to-consumer bridge translates these dense peer-reviewed findings into structured, measurable programmes for laypeople.
In the debate of Mirror Therapy vs Constraint-Induced Movement Therapy for Stroke, both modalities have their place in a 2026 neuro-rehabilitation toolkit. Mirror therapy is a gentle, accessible entry point that leverages visual feedback. CIMT is the heavy machinery required for true functional recovery.
Neuroplastic yield depends on timing, dose, and the biological substrate you provide your brain. You must activate BDNF, choose the right threshold-of-ability, and commit to the rigorous protocols that actually change brain structure.
Evidence over enthusiasm is non-negotiable. The brain you have today is not the brain you are stuck with, but you have to do the work to change it.
CIMT is generally better for long-term functional recovery because it forces the brain to overcome learned non-use through high-intensity repetition. Mirror Therapy is better for early-stage recovery when the patient has little to no active movement in the affected limb.
Yes, both can be done at home. Mirror therapy is easily set up with a simple mirror, while modified CIMT protocols use a mitt on the unaffected hand combined with targeted daily exercises. Home-based approaches are effective when protocols are rigorously structured and BDNF is activated.
Clinical protocols often use intensive schedules, sometimes up to 6 hours a day, but modified protocols show measurable progress in 2 to 4 weeks. The key is the daily repetition and forcing the brain to use the affected limb for real-world tasks.
BDNF acts as Miracle-Gro for your brain, providing the structural plasticity needed to form new neural pathways. Without sufficient BDNF, the physical repetition from therapies like CIMT will not consolidate into long-term gains.
Learned non-use occurs when a stroke survivor relies on their unaffected limb because the affected limb is difficult to move. The brain effectively stops sending signals to the affected limb, making recovery harder. CIMT directly combats this by restraining the good limb.